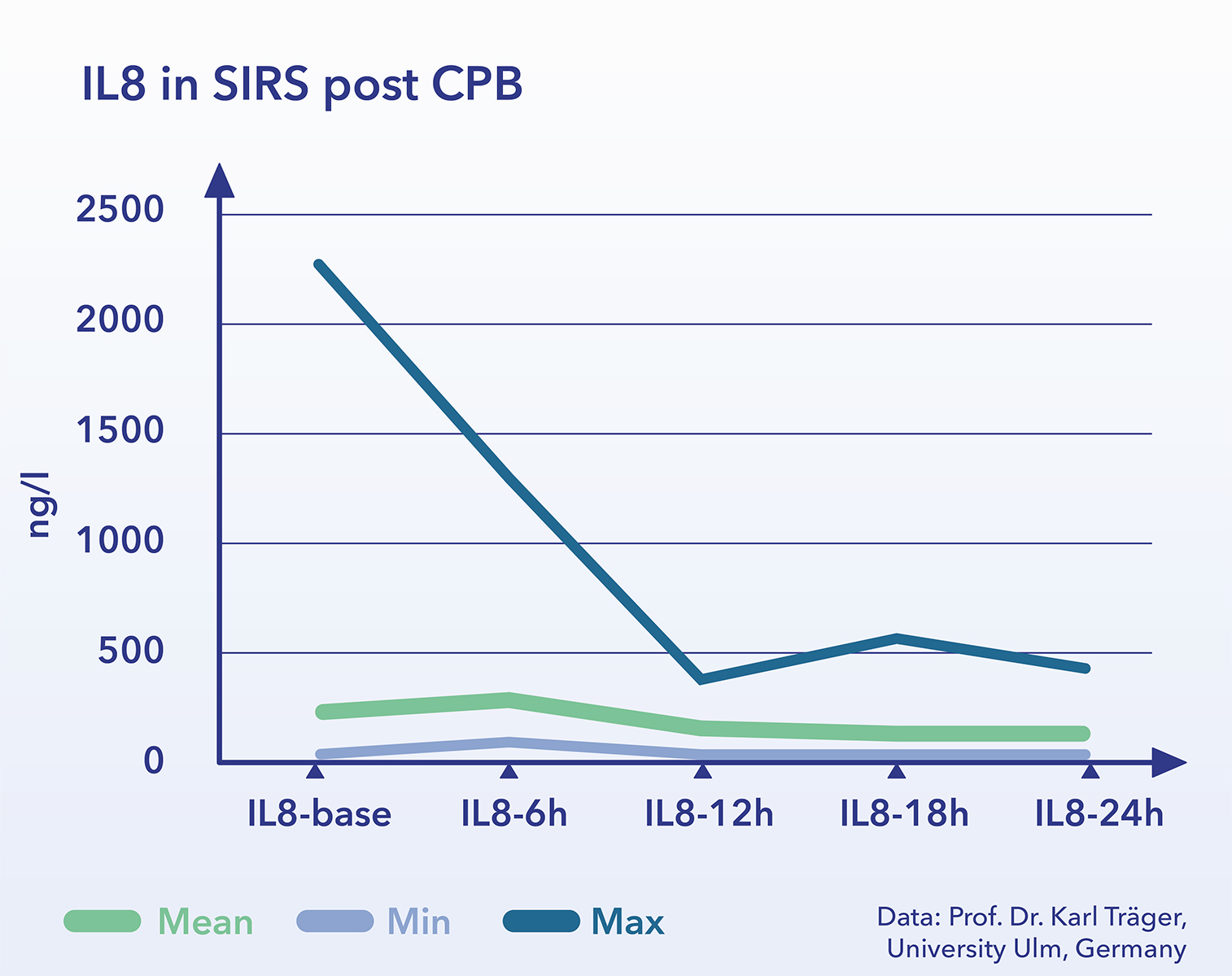
Removal of cytokines
The main focus of CytoSorb therapy* is the removal of cytokines, so inflammatory mediators, from the patient’s blood. With CytoSorb not a single defined cytokine (like e.g. IL-6) is removed, but a broad spectrum of pro- and anti-inflammatory cytokines. This is of particular importance since different messenger substances cause in part redundant effects and previous attempts to reduce individual substances have not proved to be successful.

CytoSorb provides a concentration-dependent removal based on physicochemical mechanisms. At high concentrations of a substances (e.g. cytokines) a high removal efficiency is given and large quantities can be removed very quickly. with decreasing concentrations, the removal efficiency decreases, too. This autoregulation supports to prevent complete removal of physiologic mediators like cytokines, which helps to prevent restoration of a physiologic immune response. Furthermore, while used as intended it was observed a significant removal of C3a and C5a as well as procalcitonin (Ref: 1-10).
Removal of other endogenous molecules
(e.g. myoglobin and bilirubin))
In addition to the removal of cytokines, the removal of substances that play an important role outside the systemic inflammation in the pathophysiology of certain critical diseases has also been identified in several clinical trials. These include:
Myoglobin: Acute renal failure secondary to rhabdomyolysis is the main reason for the desire to rapidly reduce high levels of myoglobin in the patient’s blood. Rhabdomyolysis, a disintegration of muscle fibers with subsequent flooding of muscle proteins and cell components, can occur in trauma, burns, infections or muscle overuse. The 17 kD molecule myoglobin can be effectively removed from the blood using CytoSorb. (Ref: 11-13)
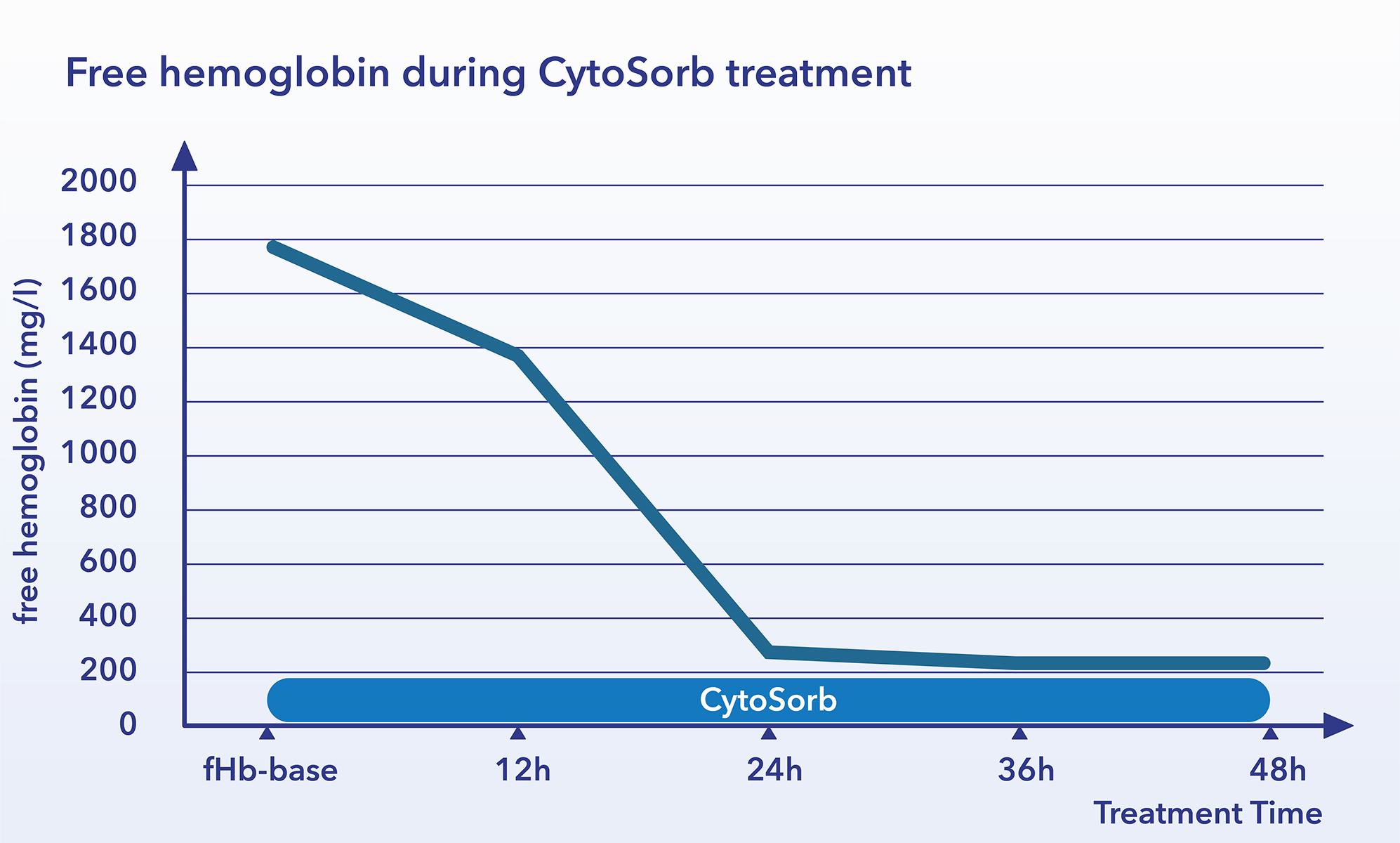
Free hemoglobin: Free hemoglobin, like free iron, is toxic. Hemoglobin released by hemolysis is normally bound to haptoglobin and then degraded. With increasing hemolysis, the binding capacity of haptoglobin is exhausted. Freeing hemoglobin can then no longer be bound and occurs freely in the plasma. Hemolyses can be triggered by mechanical influences (ECMO, HLM), infections / toxins (malaria, streptococci, EHEC), immune reactions (rhesus incompatibility) or other causes. REFRESH I clinical study observed a substantial removal of the substance from the patient’s blood can be achieved with CytoSorb. (Ref: 9)
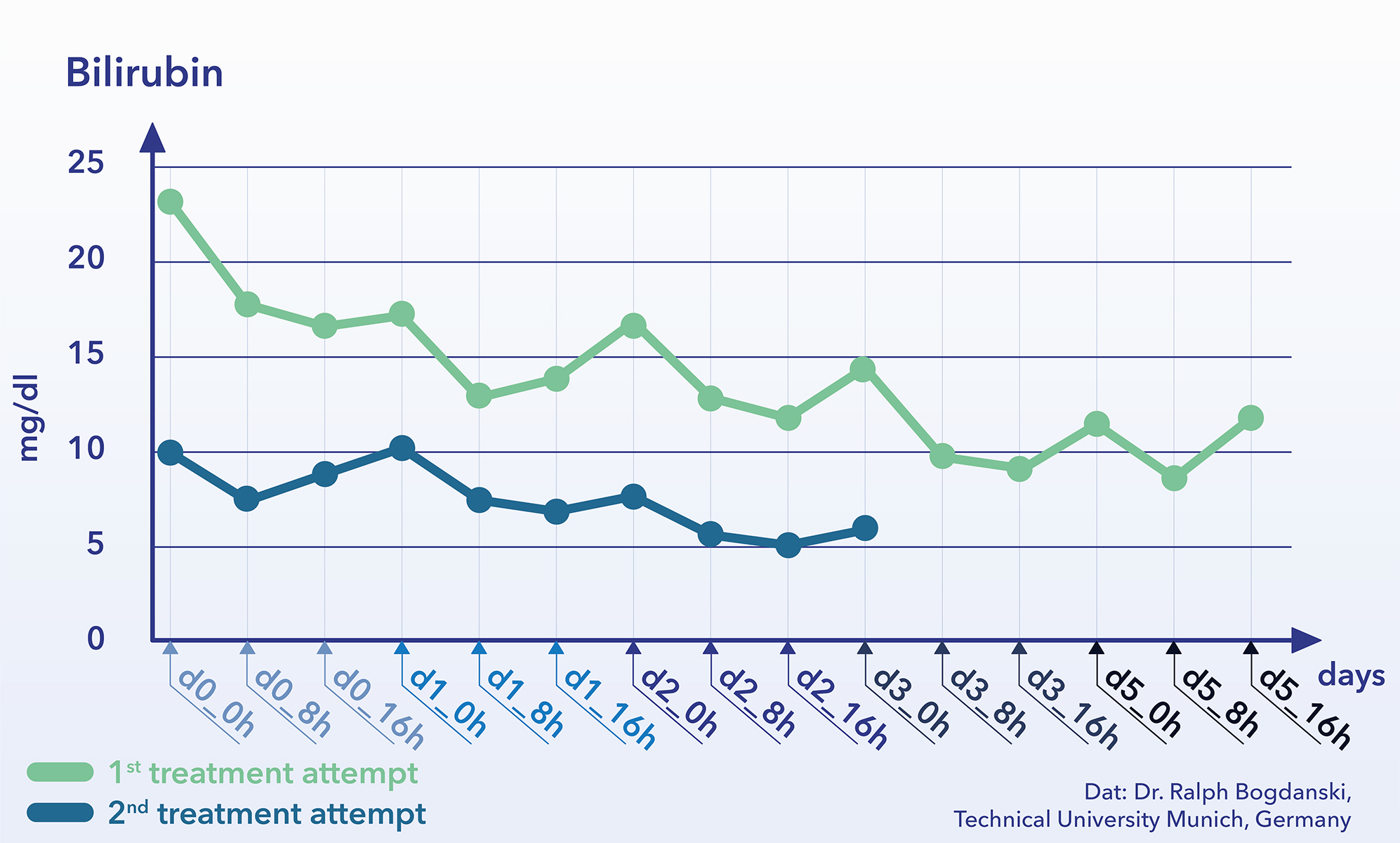
Bilirubin: Bilirubin and biliverdin are breakdown products of hemoglobin and are massively increased in the blood, if a disproportionate amount of hemoglobin is broken down by haemolysis or if accumulation occurs in the blood due to a liver function or dissolution disorder (cholestasis). Various publications have shown excellent removability of bilirubin (0.6 kDa) by CytoSorb. (Ref: 17-18)
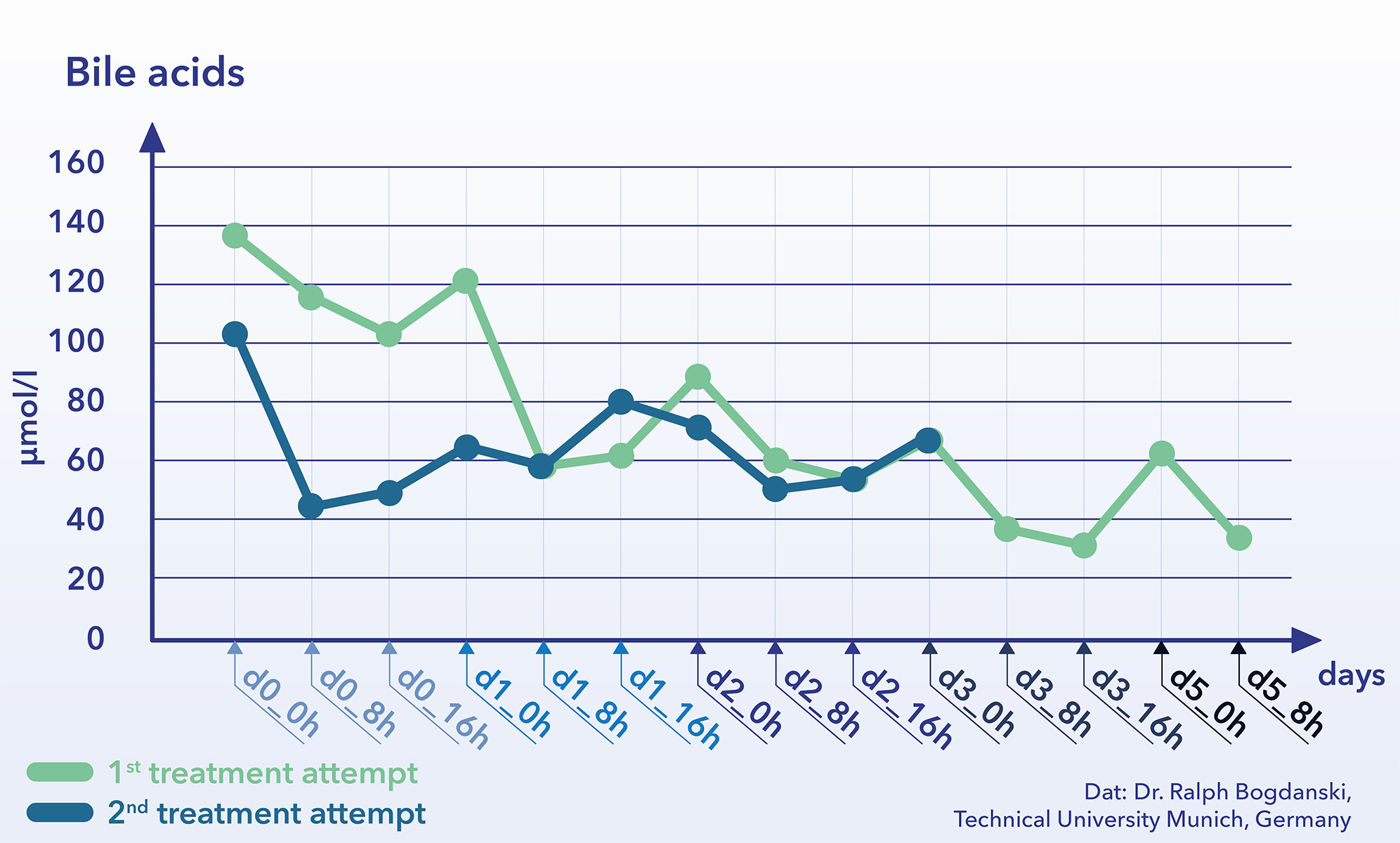
 Bile Acids: Bile acids, or their accumulation in plasma, play a significant, previously often underestimated role in critical diseases, e.g. Sepsis, systemic inflammation and liver failure. During use of CytoSorb decrease of bile acids was observed which could have the effect of prevention of toxic effects (Ref: 19).
Bile Acids: Bile acids, or their accumulation in plasma, play a significant, previously often underestimated role in critical diseases, e.g. Sepsis, systemic inflammation and liver failure. During use of CytoSorb decrease of bile acids was observed which could have the effect of prevention of toxic effects (Ref: 19).
Removal of exogenous molecules
Various preclinical and clinical investigations have observed substantial removal of the following exogenous molecules. Use of CytoSorb in an attempt to adsorb substances other than cytokines, bilirubin, myoglobin, ticagrelor, or rivaroxaban is considered off-label use and is the sole liability of the treating physician after individual risk benefit assessment. The list below, however, is also providing safety information on potential side effects and interactions by unwanted drug/substance removal.
Enterotoxins: Enterotoxins can also be used as biological weapons. It has been observed that CytoSorb quickly and safely removes a number of these toxins from the blood. (Ref: 20)
Medicines: Substances which are either intended to replace naturally occurring substances in the human body because of a deficiency, or which are to induce certain effects on account of their chemical properties, are subject to the same physical laws of transport, metabolization and excretion as endogenous substances. Like other extracorporeal blood purification methods, e.g. Dialysis or hemofiltration, CytoSorb was also observed to interact with both endogenous and exogenous molecules in the blood. The influence of CytoSorb on certain drugs should be considered when dosing and ensuring drug therapies. This can also be used to advantage in certain drugs for the removal of undesirably high plasma levels due to overdose or intoxication.
In this context, successful therapeutic trials for venlaflaxin overdoses are published. In addition, in patients who need to undergo emergency intervention while receiving treatment with P2Y12-Inhibitor Ticagrelor or Factor Xa-Inhibitor Rivaroxaban, the intraoperative removal of the substance during cardio-pulmonary bypass by CytoSorb was shown to reduce bleeding complications. (Ref: 21-26)
Removal of inflammatory mediators
(1) Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: a case series.
Trager K, Fritzler D, Fischer G, Schroder J, Skrabal C, Liebold A, Reinelt H.
Int J Artif Organs 2016; 39(3): 141-6
(2) Systemic Inflammatory Response Syndrome in der Herzchirurgie: Neue Therapiemöglichkeiten durch den Einsatz eines Cytokin-Adsorbers während EKZ?
Born F, Pichlmaier M, Peterß S, Khaladj N, Hagl C.
Kardiotechnik 2014; 2: 42-6
(3) Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model.
Peng ZY, Bishop JV, Wen XY, Elder MM, Zhou F, Chuasuwan A, Carter MJ, Devlin JE, Kaynar AM, Singbartl K, Pike F, Parker RS, Clermont G, Federspiel WJ, Kellum JA.
Crit Care 2014; 18(4): R141
(4) The effect of a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: A randomized controlled trial.
Schaedler D, Pausch C, Heise D, Meier-Hellmann A, Brederlau J, Weiler N, Marx G, Putensen C, Spies C, Jorres A, Quintel M, Engel C, Kellum JA, Kuhlmann MK.
PLoS One 2017; 12(10): e0187015
(5) Hemoadsorption Reprograms Inflammation in Experimental Gram-Negative Septic Peritonitis: Insights from In Vivo and In Silico Studies.
Namas RA, Namas R, Lagoa C, Barclay D, Mi Q, Zamora R, Peng Z, Wen X, Fedorchak MV, Valenti IE, Federspiel WJ, Kellum JA, Vodovotz Y.
Mol Med 2012; 18: 1366-74
(6) Effects of hemoadsorption on cytokine removal and short-term survival in septic rats.
Peng X, Carter M, Kellum J.A.
Crit Care Med 2008; 36(5): 1573-7
(7) Feasibility study of cytokine removal by hemoadsorption in brain-dead humans.
Kellum JA, Venkataraman R, Powner D, Elder M, Hergenroeder G, Carter M.
Crit Care Med 2008; 36(1): 268-72
(8) Hemoadsorption removes tumor necrosis factor, interleukin-6, and interleukin-10, reduces nuclear factor-кB DNA binding, and improves short-term survival in lethal endotoxemia.
Kellum JA, Song M, Venkataraman R.
Crit Care Med 2004; 32(3): 801-5
(9) Hemoadsorption to Reduce Plasma Free Hemoglobin during Cardiac Surgery: Results of REFRESH I Pilot Study.
Gleason TG, Argenziano M, Bavaria JE, Kane LC, Coselli JS, Engelman RM, Tanaka KA, Awad A, Sekela ME, Zwischenberger JB.
Semin Thorac Cardiovasc Surg 2019; 31(4): 783-93
(10) Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study.
Hawchar F, László I, Öveges N, Trásy D, Ondrik Z, Molnar Z.
Journal of Critical Care 2019; 49: 172-8
Removal of other endogenous molecules
Ecstasy
(11) Use of the CytoSorb adsorption device in MDMA intoxication: a first-in-man application and in vitro study.
Lang CN, Sommer MJ, Neukamm MA, Staudacher DL, Supady A, Bode C, Duerschmied D, Lother A.
Intensive Care Med Exp 2020; 8(1): 21
(12) Venlafaxine intoxication with development of takotsubo cardiomyopathy: successful use of extracorporeal life support, intravenous lipid emulsion and CytoSorb(R).
Schroeder I, Zoller M, Angstwurm M, Kur F, Frey L .
Int J Artif Org 2017; 40(7): 358 – 60
Amitriptyline:
(13) Use of CytoSorb in cases of acute amitriptyline intoxication.
Paland M.
J Clin Pharm Ther 2021; epub
Myoglobin
(14) Blood purification with a cytokine adsorber for the elimination of myoglobin in critically ill patients with severe rhabdomyolysis.
Scharf C, Liebchen U, Paal M, Irlbeck M, Zoller M, Schroeder I.
Crit Care 2021; 25(1): 41
(15) Cytosorb™ in a patient with legionella-pneumonia associated rhabdomyolysis.
Wiegele M, Krenn CG.
ASAIO J 2015; 61(3): e14-6
(16) In-Vitro Myoglobin Clearance by a Novel Sorbent System.
Kuntsevich VI, Feinfeld DA, Audia PF, Young W, Capponi V, Markella M, Winchester JF.
Artificial Cells, Blood Substitutes, & Biotechnology 2009; 37: 45-7
Bilirubin
(17) Successful elimination of bilirubin in critically ill patients with acute liver dysfunction using a cytokine adsorber and albumin dialysis: a pilot study.
Scharf C, Liebchen U, Paal M, Becker-Pennrich A, Irlbeck M, Zoller M, Schroeder I.
Sci Rep 2021; 11(1): 10190
(18) Removal of Bilirubin with a New Adsorbent System: In Vitro Kinetics.
Gemelli C, Cuoghi A, Magnani S, Atti M, Ricci D, Siniscalchi A, Mancini E, Faenza S.
Blood Purif 2019; 47(1): 10-5
Bile acids
(19) Removal of bile acids by extracorporeal therapies: an in vitro study.
Hartmann J and Harm S.
Int J Artif Organs 2017; 40(1): 4–8
Removal of exogenous molecules – enterotoxins
(20) Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb(R) sorbent porous polymer beads.
Gruda MC, Ruggeberg KG, O’Sullivan P, Guliashvili T, Scheirer AR, Golobish TD, Capponi VJ, Chan PP.
PLoS One 2018; 13(1): e0191676
Removal of exogenous molecules – drugs
(21) Pharmacokinetics of anti-infective agents during CytoSorb hemoadsorption
Schneider AG, Andre P, Scheier J, Schmidt M, Ziervogel H, Buclin T, Kindgen-Milles D.
Sci Rep 2021; 11(1): 10493
(22) Ticagrelor Removal From Human Blood.
Angheloiu GO, Gugiu GB, Ruse C, Pandey R, Dasari RR, Whatling C.
JACC: Basic to Translational Science 2017; 2(2): 135–145
(23) Extracorporeal Hemoperfusion as a Potential Therapeutic Option for Critical Accumulation of Rivaoxaban.
Koertge A, Wasserkort R, Wild T, Mitzner S.
Blood Purification 2018; 45: 126–8
(24) Cytosorb adsorption during emergency cardiac operations in patients at high risk of bleeding.
Hassan K, Kannmacher J, Wohlmuth P, Budde U, Schmoeckel M, Geidel S.
Annals of Thoracic Surgery 2019; 108(1); 45–51
(25) Venlafaxine intoxication with development of takotsubo cardiomyopathy: successful use of extracorporeal life support, intravenous lipid emulsion and CytoSorb.
Schroeder I, Zoller M, Angstwurm M, Kur F, Frey L.
Int J Artif Organs 2017; 40(7): 358-60
(26) First-in-Man Fully Percutaneous Complete Bypass of Heart and Lung.
Napp LC, Vogel-Claussen J, Schäfer A, Haverich A, Bauersachs J, Kühn C, Tongers J.
JACC Cardiovasc Interv 2017; 10(24): e231–3
Attenuation of the excessive acute phase reaction
The acute phase reaction is a nonspecific immune response of the body and part of the inflammatory response. An excessive acute phase response is associated with a number of potential complications.
These relate in particular to coagulation and microcirculation disorders with consequent deterioration of tissue oxygenation and secondary organ dysfunction due to impaired homeostasis. The attenuation of an excessive acute phase reaction by removal of elevated levels of cytokines is the primary approach with CytoSorb therapy. (Ref: 1-5)
Reduction of cytokine production
The clinical effects of CytoSorb therapy are only partially based on the direct removal of cytokines and chemokines. Several studies have shown that Cytosorb can remove Cytokines which has been observed to help to regain control during the cytokine storm. On one hand, this is made possible by the lower plasma levels of pro-inflammatory cytokines, since these can have a self-reinforcing effect on new production; on the other hand, molecules that sustain the inflammatory cascade are removed. (Ref: 5-9)
References
Attenuation of the excess acute phase reaction
(1) Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: a case series
Trager K, Fritzler D, Fischer G, Schroder J, Skrabal C, Liebold A, Reinelt H
Int J Artif Organs 2016; 39(3): 141-146
(2) Systemic Inflammatory Response Syndrome in der Herzchirurgie: Neue Therapiemöglichkeiten durch den Einsatz eines Cytokin-Adsorbers während EKZ?
Born F, Pichlmaier M, Peterß S, Khaladj N, Hagl C
Kardiotechnik 2/2014
(3) Feasibility study of cytokine removal by hemoadsorption in brain-dead humans
Kellum JA, Venkataraman R, Powner D, Elder M, Hergenroeder G, Carter M
Crit Care Med. 2008 Jan;36(1):268-7
(4) Effects of hemoadsorption on cytokine removal and short-term survival in septic rats
Peng X, Carter M, Kellum J.A.
Crit Care Med. 2008 May;36(5):1573-7
(5) Cytokine and DAMP adsorption in septic acute kidney injury
C.M. Laubach, K.-P. Janssen, W. Johannes, R. Bogdanski, B. Kapfer
Intensive Care Medicine Experimental 2018, 6(Suppl 2):0627
Reduction of cytokine production
(6) Hemoadsorption removes tumor necrosis factor, interleukin-6, and interleukin-10, reduces nuclear factor-кB DNA binding, and improves short-term survival in lethal endotoxemia
Kellum JA, Song M, Venkataraman R
Crit Care Med. 2004 Mar;32(3):801-5
Realignment of activated leukocytes
(7) Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model
Peng ZY, Bishop JV, Wen XY, Elder MM, Zhou F, Chuasuwan A, Carter MJ, Devlin JE, Kaynar AM, Singbartl K, Pike F, Parker RS, Clermont G, Federspiel WJ, Kellum JA
Crit Care 2014, 18(4):R141
(8) Hemoadsorption reprograms inflammation in experimental gram-negative septic peritonitis: insights from in vivo and in silico studies.
Namas RA, Namas R, Lagoa C, Barclay D, Mi Q, Zamora R, Peng Z, Wen X, Fedorchak MV, Valenti IE, Federspiel WJ, Kellum JA, Vodovotz, Y.
Mol Med 2012; 18:1366-74.
(9) Acute removal of common sepsis mediators does not explain the effects of extracorporeal blood purification in experimental sepsis
Peng ZY, Wang HZ, Carter MJ, Dileo MV, Bishop JV, Zhou FH, Wen XY, Rimmelé T, Singbartl K, Federspiel WJ, Clermont G, Kellum JA
Kidney Int. 2012 Feb;81(4):363-9
The clinical effects of using CytoSorb therapy are highly dependent on the indication, the clinical situation and the treatment regimen. The therapy is not to be used as a last resort treatment treatment, but rather for its positive clinical effects, especially with careful patient selection, timely use and appropriate use. Existing therapeutic principles, such as focal source removal and early anti-infective therapy in sepsis remain of utmost importance. Goals for the use of CytoSorb therapy are the aimed at the following clinical effects:
Support of hemodynamic stabilization
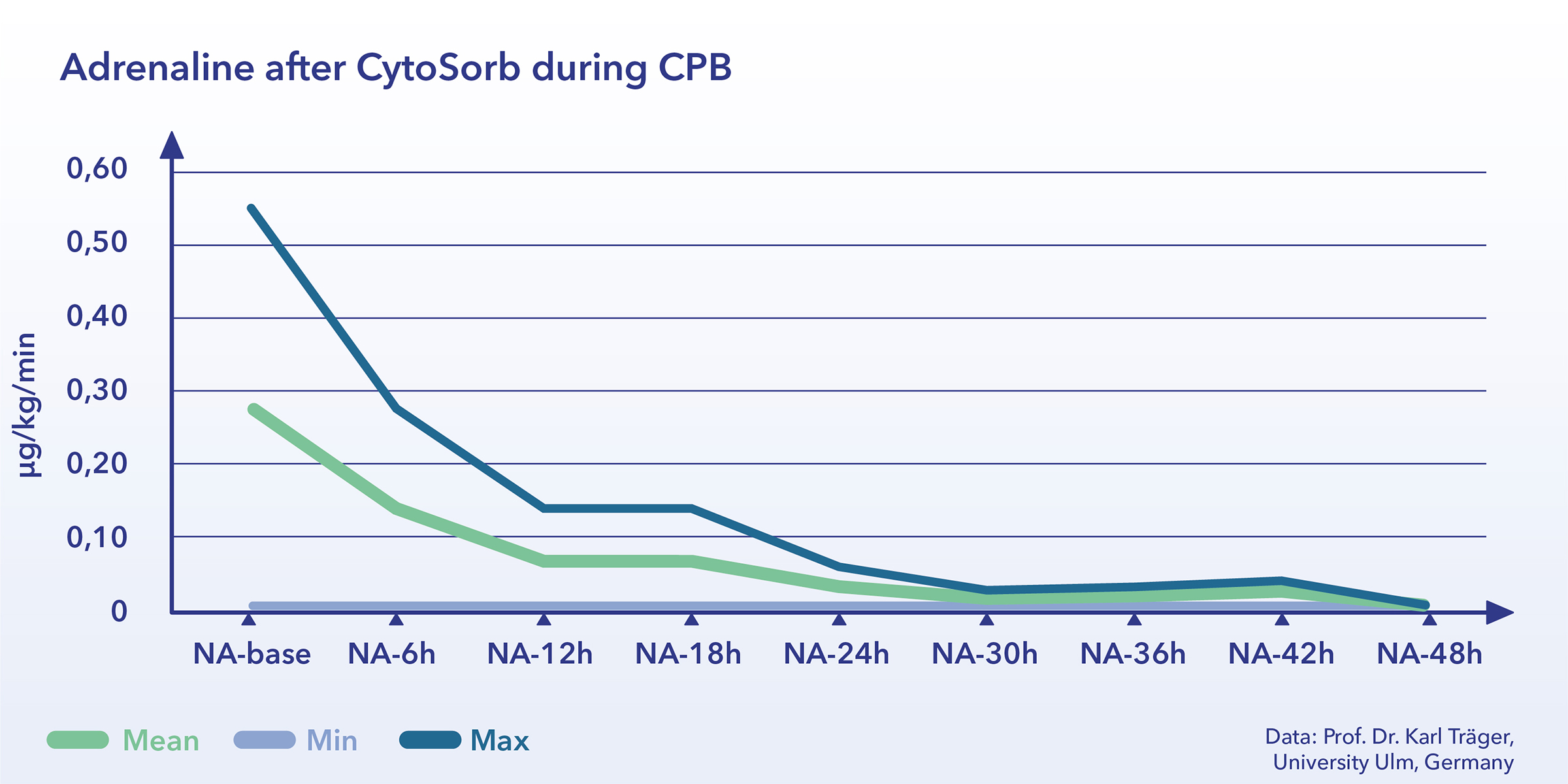
A frequently described an reproducible effects observed from the removal of cytokines with significant decreases in vasopressor needs as observed in clinical investigations. (Ref: 1-11)
Influence on capillary leak
The reduction in systemic peak cytokine levels might also reduce their impact on the vascular integrity. In preclinical studies, the group led by Dr John Kellum of Pittsburgh (USA) clearly demonstrated this effect, and in vitro measurements on human endothelial cell layers with untreated and treated plasma have tentatively confirmed this. Even previous clinical observations appear to confirm these results. By removing excess cytokines, CytoSorb can help the body potentially stops the passage of fluid, proteins, and immune cells into various tissues and prevents the progression of organ damage. At the same time, the improvement of organ function has been observed may also be promoted by these effects. (Ref: 12-18)
Organ protection and treatment of multi-organ dysfunction
Organ protection can be achieved in different clinical situations and through different mechanisms of action. For example, the consistent reduction of high plasma levels of myoglobin using CytoSorb might help to mitigate or even prevent renal insufficiency
helps prevent renal insufficiency secondary to rhabdomyolysis. A similar effect might be expected from the massive removal of free hemoglobin in cases of significant hemolysis. The removal of potentially cytotoxic substances such as bile acids, can support liver detoxification function.
Multi-organ dysfunction or failure (lung, kidney, liver, heart, circulation, etc.) are common complications of severe or excessive systemic inflammatory reactions. Dampening of the so-called cytokine storm by the CytoSorb therapy is meant to support prevention or mitigation of organ failure. If the organ dysfunction is exclusively the result of inflammation and not due to subsequent onset cell damage, the organ function might also recover after systemic inflammation has been dampened. Studies trying to confirm these effects in the clinical setting are currently in progress.
Re-direction of cellular immune defense
A potential additional therapeutic approach would be based on influencing the cellular immune response by lowering cytokine levels in the patient’s blood. This may “unmask” an existing infectious focus, as the local mediator levels remain high despite a reduction in systemic levels. The resulting concentration gradient of the inflammatory mediators between focus and periphery could reorient the previously undirected, systemic cellular immune response to the focus. Dr Peng and coworkers were able to show this preclinically. Confirmation under clinical conditions is currently being sought. (Ref: 17-18)

Prevention or mitigation of excess systemic inflammation under extracorporeal circulation
Study results in cardiac surgery patients show that the use of CytoSorb therapy might prevent or significantly reduce systemic inflammation due to the use of the heart-lung machine (HLM). This has previously been seen in pre-clinical projects. The lack of, or greatly reduced, systemic inflammation might then induce less complications, such as hemodynamic instability or secondary organ dysfunction. The precise setting in which this approach is best used is still under investigation. (Ref 21-22)
References
Stabilization of hemodynamics (micro and macro circulation)
(1) Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: a case series
Trager K, Fritzler D, Fischer G, Schroder J, Skrabal C, Liebold A, Reinelt H
Int J Artif Organs 2016; 39(3): 141-146
(2) Combination of ECMO and cytokine adsorption therapy for severe sepsis with cardiogenic shock and ARDS due to Panton-Valentine leukocidin-positive Staphylococcus aureus pneumonia and H1N1
Lees NJ, Rosenberg A, Hurtado-Doce AI, Jones J, Marczin N, Zeriouh M, Weymann A, Sabashnikov A, Simon AR, Popov AF
J Artif Organs 2016 epub
(3) Septic shock secondary to β-hemolytic streptococcus-induced necrotizing fasciitis treated with a novel cytokine adsorption therapy.
Hetz H, Berger R, Recknagel P, Steltzer H.
Int J Artif Organs. 2014 37(5): 422-6
(4) CytoSorb, a novel therapeutic approach for patients with septic shock: a case report
Hinz B, Jauch O, Noky T, Friesecke S, Abel P, Kaiser R
Int J Artif Organs 2014 38(8): 461-46
(5) First description of SPAD combined with cytokine adsorption in fulminant liver failure and hemophagocytic syndrome due to generalized HSV-1 infection.
Frimmel S, Schipper J, Henschel J, Yu TT, Mitzner SR, Koball S.
Liver Transpl. 2014 Dec;20(12):1523-4
(6) Use of a novel hemoadsorption device for cytokine removal as adjuvant therapy in a patient with septic shock with multi-organ dysfunction: A case study
Basu R, Pathak S, Goyal J, Chaudhry R, Goel RB, Barwal A
Indian J Crit Care Med 2014;18:822-4
(7) Effects of a novel cytokine haemoadsorbtion system on inflammatory response in septic shock after cephalic pancreatectomy – a case report
Tomescu D, Dima SO, Tănăsescu S, Tănase CP, Năstase A , Popescu M
Romanian Journal of Anaesthesia and Intensive Care 2014;21(2):134-138
(8) Improvement of hemodynamic and inflammatory parameters by combined hemoadsorption and hemodiafiltration in septic shock: a case report.
Mitzner SR, Gloger M, Henschel J, Koball S
Blood Purif. 2013;35(4):314-5.
(9) Effects of hemoadsorption on cytokine removal and short-term survival in septic rats
Peng ZY, Carter MJ, Kellum JA
Crit Care Med. 2008 May;36(5):1573-7
(10) Hemoadsorption removes tumor necrosis factor, interleukin-6, and interleukin-10, reduces nuclear factor-кB DNA binding, and improves short-term survival in lethal endotoxemia
Kellum JA, Song M, Venkataraman R
Crit Care Med. 2004 Mar;32(3):801-5
(11) Extracorporeal Cytokine Elimination as Rescue Therapy in Refractory Septic Shock – a Prospective Single-Center Study
Friesecke S, Stecher SS, Gross S, Felix SB, Nierhaus A.
Journal Artif Organs 2017; 20(3): 252-9
Influence on capillary leak
(12) Cytokine Reduction in the Setting of an ARDS-Associated Inflammatory Response with Multiple Organ Failure
Trager K, Schutz C,Fischer G, Schroder J, Skrabal C, Liebold A, Reinelt H
Case Rep Crit Care 2016: 9852073
(13) CytoSorb, a novel therapeutic approach for patients with septic shock: a case report
Hinz B, Jauch O, Noky T, Friesecke S, Abel P, Kaiser R
Int J ArtifOrgans. 2015 Sep 18;38(8):461-4
(14) Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model.
Peng ZY, Bishop JV, Wen XY, Elder MM, Zhou F, Chuasuwan A, Carter MJ, Devlin JE, Kaynar AM, Singbartl K, Pike F, Parker RS, Clermont G, Federspiel WJ, Kellum JA.
Crit Care. 2014 Jul 3;18(4):R141
(15) Effect of cytokine hemoadsorption on brain death-induced ventricular dysfunction in a porcine model.
Mikhova KM, Don CW, Laflamme M, Kellum JA, Mulligan MS, Verrier ED, Rabkin DG
J Thorac Cardiovasc Surg. 2013 Jan;145(1):215-24
(16) Hemoadsorption Reprograms Inflammation in Experimental Gram-Negative Septic Peritonitis: Insights from In Vivo and In Silico Studies.
Namas RA, Namas R, Lagoa C, Barclay D, Mi Q, Zamora R, Peng Z, Wen X, Fedorchak MV, Valenti IE, Federspiel WJ, Kellum JA, Vodovotz Y
Mol Med. 2012 Dec 20;18:1366-74
(17) Acute removal of common sepsis mediators does not explain the effects of extracorporeal blood purification in experimental sepsis
Peng ZY, Wang HZ, Carter MJ, Dileo MV, Bishop JV, Zhou FH, Wen XY, Rimmelé T, Singbartl K, Federspiel WJ, Clermont G, Kellum JA
Kidney Int. 2012 Feb;81(4):363-9
(18) Effect of extracorporeal cytokine removal on vascular barrier function in a septic shock patient
S. David, K. Thamm, B. M. W. Schmidt, C. S. Falk and J. T. Kielstein
Journal of Intensive Care (2017) 5:12
Re-direction of cellular immune defense
(19) Hemoadsorption Reprograms Inflammation in Experimental Gram-Negative Septic Peritonitis: Insights from In Vivo and In Silico Studies.
Namas RA, Namas R, Lagoa C, Barclay D, Mi Q, Zamora R, Peng Z, Wen X, Fedorchak MV, Valenti IE, Federspiel WJ, Kellum JA, Vodovotz Y
Mol Med. 2012 Dec 20;18:1366-74
(20) Modulation of chemokine gradients by apheresis redirects leukocyte trafficking to different compartments during sepsis, studies in a rat model.
Peng ZY, Bishop JV, Wen XY, Elder MM, Zhou F, Chuasuwan A, Carter MJ, Devlin JE, Kaynar AM, Singbartl K, Pike F, Parker RS, Clermont G, Federspiel WJ, Kellum JA.
Crit Care. 2014 Jul 3;18(4):R141
Prevention or slowing down of excessive systemic inflammation
(21) Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: a case series
Trager K, Fritzler D, Fischer G, Schroder J, Skrabal C, Liebold A, Reinelt H
Int J Artif Organs 2016; 39(3): 141-146
(22) Systemic Inflammatory Response Syndrome in der Herzchirurgie: Neue Therapiemöglichkeiten durch den Einsatz eines Cytokin-Adsorbers während EKZ?
Born F, Pichlmaier M, Peterß S, Khaladj N, Hagl C
Kardiotechnik 2/2014